The next step after recognizing an issue is knowing where to find the answer. Does your issue really violate good infection control practices and patient safety? You need to know your resources, but you don't need to memorize every one. Google is my best friend. Because the problem you are facing is not likely the first occurrence of said problem in the history of modern healthcare, there is information out there somewhere on it. Often my search leads directly to one of the published guidelines, and then I don’t have to know exactly which one it is off-hand. I find the CDC MDRO and Precautions guidelines overlap a lot, and the SHEA compendium overlaps APIC. So if you are looking for exact wording on your issue without reading through each one, just do an internet search with as many key words as you can.
Over the years, I’ve collected (and I’m sure many ICPs have) a number of photos of things that didn’t look right.
Exhibit 1:

This is a feeding pump. Staff let the pediatric patients decorate it with adhesive stickers to make it look it more friendly. Does it look not-quite-right to you? It should. All of that adhesive attracts debris, and you can’t clean adhesive. In fact, those stickers are debris. Feeding fluids are full of sugars, proteins, and other nutrients that are great for feeding humans and bacteria. There should not be adhesives on patient care items. Reference: CDC Guideline for Cleaning and Disinfection
Exhibit 2:

This is drinks at the nursing station. I count 3 from this angle. Along with a personal bag. We use this counter to put laboratory specimens, patient charts (gross), glcuometers, etc. It is not a clean area. Staff should have a clean area for food and drinks in a non-clinical space, and should have a work flow that allows for breaks for their own fluid intake. This is up to the manager to police and enforce. I always find more drinks after-hours than during the day. Reference: OSHA blood borne pathogen standard.
Exhibit 3:

This is an isolation gown, hanging on the doorknob, ready to be worn again….. Does it look wrong? If you don’t see dozens of gowns on doorknobs, then one should strike you as an aberrancy, something out of the ordinary. Isolation gowns are worn once. They are considered contaminated once worn, and you would not be able to put it on again without recontaminating yourself. This is wrong. Reference: CDC Guideline for Isolation Precautions.
Exhibit 4:

I didn’t take this photo; an environmental services manager did, and brought it to me. He said, “Can they leave the ceiling open?” No, they can’t. This is open for work being done in a patient room. He walked by the room and the door was open, and no worker was nearby. As the room is empty, it’s likely been cleaned. Does the Facilities staff know they need to contain debris from the ceiling in a patient area? That a ladder and open tiles shouldn’t be unattended? Does the nursing staff know that they can’t just push the bed back in there, as the room needs to be cleaned again? This is the result of poor project planning: Nursing needs to know what work is being done, Facilities needs to know how to do it safely, and everyone, including EVS, needs to be sure the room is clean after.
Exhibit 5:
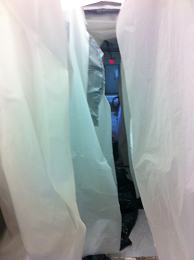
What’s this? I wish it was a better pic. But this is several layers of plastic (soft) containment set up during major construction in a hospital. Is something wrong here? Why, yes. I can see the glowing exit sign at the end of the hallway they are working in. This is 2 layers of containment, both open, gently blowing in the breeze, so that a person on the safe side with a camera can actually see all the way through the demolition area to the other end. Unacceptable. Containment is for containing debris and air contaminants, and protecting patients and staff. This is doing neither. This is where you may wield your authority, and tell the contractor to stop work until the containment is fixed. Speak to your Facilities director immediately, as they are responsible for ensuring contractors are properly trained in infection control measures, and have ultimate responsibility for ensuring it happens. Reference for both above: CDC Guidelines for Environmental Infection Control in Health Care Facilities
So if you wander about your facility and see something that doesn’t look quite right or something you’ve not seen in other facilities, trust your gut: it’s probably wrong. Head back to your office, find your reference, and then go correct the problem like the infection-preventing deity you are.